Inside the science of endometriosis-associated pain
An Interview with Eleonora Persoons from the Vriens/Voets Lab and Vaidi Plovie from Endo.Insideout vzw
March marks Endometriosis Awareness Month, a time when the experiences of millions of people living with this condition are given the visibility they deserve. We interview Eleonora Persoons, who works in close collaboration between the labs of Joris Vriens, Thomas Voets, and the fertility center at UZ Leuven. Her research offers a rare and much‑needed window into the molecular mechanisms that drive endometriosis‑associated pain. We also chat with Vaidi Plovie, who founded the patient organization Endo.Insideout, and shares her experience of living with endometriosis. Discover how Eleonora is helping to bridge patient care and fundamental science, and why her work matters in a field where progress has long been slowed by stigma, biological complexity, and a striking lack of research.
Endometriosis is...
- a chronic inflammatory condition in which tissue similar to the uterine lining grows outside the uterus, causing lesions, scarring, and sometimes organ adhesions. This can lead to persistent inflammation, nerve growth, and immune disruption
- characterized by symptoms such as severe pelvic pain, painful periods, pain during sex, gastrointestinal issues, fatigue, and fertility problems.
- affecting around 10% of reproductive-age people with a uterus, even though the condition remains widely under‑recognized, with diagnostic delays of 5 to 12 years due to symptom dismissal, variability, and the lack of non‑invasive tests. This delay often worsens disease progression and has a profound impact on quality of life, influencing mobility, work, relationships, sleep, and mental well‑being.
Endometriosis didn’t just affect parts of my life; it slowly took over everything. For years, I lived in a body that constantly felt like it was working against me. I was in pain more often than not, but I kept going. I went to school, I worked, I tried to be present for friends and family… but behind the scenes, I was surviving rather than living.
- Vaidi Plovie
Meet Eleonora Persoons, an endometriosis researcher whose work bridges clinical insight with fundamental mechanistic research. She’s currently doing her postdoc in the labs of Joris Vriens at KU Leuven. Her co‑promoter, Thomas Voets, leads one of the labs at the VIB-KU Leuven Center for Neuroscience, where the focus lies on the molecular logic of sensory transduction — particularly the ion channels that allow cells to detect various stimuli, including pain. Her path into this field began years earlier, during her master’s thesis with Vriens.
“When choosing the topic for my master’s thesis, I wanted to do something in the field of gynaecology. At the same time, I’ve also always had an interest in neuroscience, but that couldn’t be integrated in my Master’s thesis at the time.” As she began considering a PhD, the two threads finally converged. Vriens mentioned that he had long hoped to launch a project on endometriosis and pain, supported by the lab’s close collaboration with the fertility center. “Because this involved an element of studying pain, it blended both of my research interests perfectly,” Eleonora says. “It’s been the best of both worlds!”

Rethinking pain pathways in endometriosis
Building on their deep foundation in pain physiology, Eleonora and the team began to look for molecular clues that might explain why endometriosis pain is so persistent and difficult to treat.
“Most endometriosis patients report a lot of pain symptoms, so we started wondering whether one of the ion channels that we study in the Voets Lab — which is already known to be involved in inflammatory pain — might also be linked to endometriosis,” Eleonora explains.
Most existing research into the molecular basis of endometriosis has focused on TRPV1, the first of the TRP family of ion channels to be discovered in 1997. [Editor's note: Transient Receptor Potential channels are 'tunnels' in the membrane of animal cells that relay molecular signals.] However, previous studies show that this channel is not a good therapeutical target, due to failure in clinical trials and severe side effects such as hyperthermia.
"We decided to broaden our research to other TRP channels," Eleonora recalls. "Endometriosis depends on oestrogen, and lesions caused by endometriosis can make their own oestrogen from cholesterol. In doing so, they also produce early steroid precursors like pregnenolone sulphate — a strong activator of the TRPM3 ion channel. This means TRPM3 could be switched on directly within the lesion environment."
Crucially, the Vriens lab together with the Voets Lab have shown that TRPM3 is not just another TRP channel, but a key molecular sensor for noxious heat and inflammatory pain. They also found that its activity becomes heightened in chronic pain states, and that blocking TRPM3 can reduce pain behaviours in models of neuropathic and inflammatory pain.
A reliable model
One of the biggest barriers in Eleonora’s work is the challenge of building a reliable research model for endometriosis to study innervation and pain symptoms.
“Because endometriosis only occurs in species that menstruate, we first have to induce artificial menstruation in laboratory animals, as only humans, a few primates, some bats, elephant shrews, and the Egyptian spiny mouse menstruate,” she explains.
Endometriotic lesions are thought to form through retrograde menstruation, which occurs when menstrual tissue flows backward into the pelvic cavity. This is a natural process, but in about 10% of menstruating individuals, the menstrual tissue in the abdomen will attach and develop into lesions. “If you want to mimic that in the lab, you first need menstrual tissue,” she says. Thankfully, a model to induce endometriosis in mice already exists: after a three‑week protocol, the menstrual tissue can be collected and injected into a recipient animal’s abdomen.

"Before conducting additional experiments, we must allow time for biological processes to develop," Eleonora says. "After all, nerve connections do not form instantly, so the lesions are left to grow for about twelve weeks. Over this period, they attach to surrounding tissue and develop a network of nerve fibers, which makes them suitable for detailed study outside the body."
While similar models have been used in the past, earlier studies did not wait long enough to observe this level of nerve growth. A key innovation that Eleonora introduced is the use of genetically engineered mice, which makes it possible to selectively visualize the nerve fibers growing into the lesions.
"Using this endometriosis model, we found clear evidence that two ion channels (TRPM3 and TRPV1) are active in the nerve fibers that grow into endometriotic lesions," explains Eleonora. "This is important because identifying the specific sensors involved in detecting pain creates new opportunities to develop treatments that can block these signals."
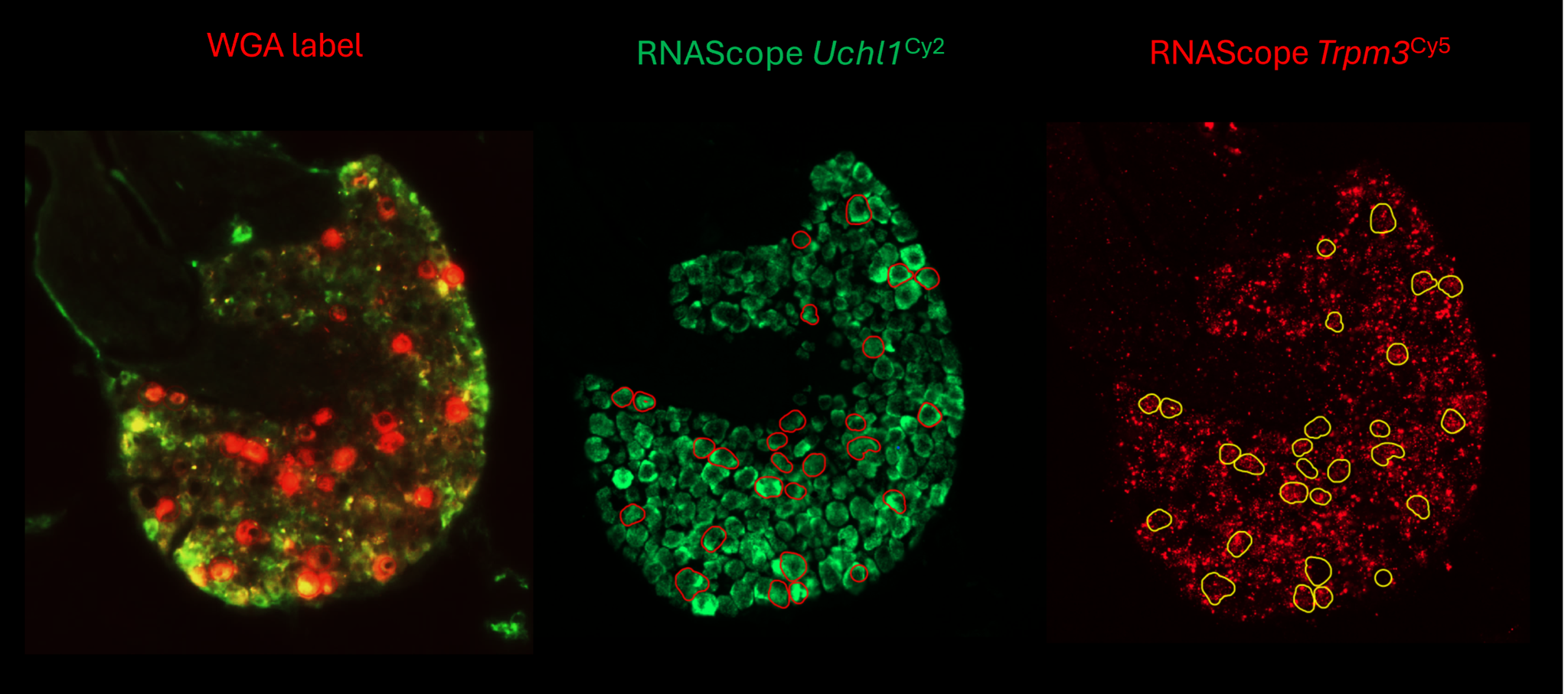
The team also used advanced techniques (like the RNAScope in the header image) to trace and analyze the neurons connected to these lesions. They discovered that TRPM3 is produced at higher levels in these nerve cells compared to those in healthy animals. This suggests that the inflammatory environment associated with endometriosis may directly alter how pain is processed in the body.
In addition, Eleonora developed a new research model in rats that mimics endometriosis-like symptoms. "This model offers important advantages, as rats can display a wider and more detailed range of pain-related behaviors than mice, making them especially useful for testing potential treatments in early-stage studies."
Bridging patient care and molecular science
In the lab of Joris Vriens, there is a close partnership with UZ Leuven and the clinicians who diagnose and treat endometriosis, creating a rare bridge between molecular research and patient care. Together, they have already completed The ExPAND Study, which examined the presence of neurosteroid‑related enzymes and TRPM3‑linked steroid precursors in human endometriosis lesions.
The team found that patients with the most severe pain symptoms showed an upregulation of one of the enzymes responsible for producing steroid molecules in the endometrium. This finding suggests that the local production of steroid precursors — known to activate TRPM3 — may indeed play a role in the pain mechanisms of endometriosis. In other words, the human data reinforce the emerging hypothesis from Eleonora’s mechanistic work: that steroid‑driven activation of TRPM3 could be a meaningful contributor to endometriosis‑associated pain.

to determine the exact DRG neurons that innervate the lesion.
One of the most painful parts of my journey was not being believed. I was told, directly and indirectly, that what I was experiencing was 'normal'; that period pain is something women just have to deal with. So I started questioning myself. Maybe I was exaggerating. That’s what a long diagnostic process does to you; it erodes your trust in yourself.
There are incredible healthcare professionals who truly listen and make a difference. In my experience, there is still too little knowledge about the full picture of endometriosis. We try to bridge that gap with Endo.Insideout by working together with healthcare professionals and spreading more accurate information.
- Vaidi Plovie
The silent barriers to a breakthrough
Beyond the technical challenges of modelling the disease, Eleonora faces a broader landscape of structural and cultural barriers that slow progress in endometriosis research. In Belgium, the research field remains strikingly small; at KU Leuven, only one other research group is actively studying the condition at a fundamental level.
Furthermore, the disease’s biological diversity also makes understanding and treating endometriosis difficult: some patients develop peritoneal lesions, others deep infiltrating lesions, others ovarian lesions, and many have a combination. Pain symptoms vary just as widely.
“Pain is so subjective,” Eleonora explains. “What one person rates as a five, another might rate as a ten. No two people experience endometriosis in the same way, and that makes it incredibly difficult to study.
Cultural stigma adds another layer of complexity. The taboo surrounding menstruation still shapes how society talks — or doesn’t talk — about the condition. “Menstruation is still a taboo topic,” Eleonora admits. “I’ve been in conversations with scientists who are uncomfortable talking about menstruation and pelvic pain symptoms.”
This silence has consequences: people often don’t know what counts as 'normal', or when their symptoms warrant medical attention. And even when they do seek help, they may not be taken seriously, as severe period pain is still widely dismissed as something to endure rather than investigate.
Endo.Insideout was born out of everything I missed during my own journey. I never want someone to feel as alone and unheard as I did. We focus on visibility, storytelling, and connection. We create safe spaces where people can share their experiences without shame or doubt. Because the moment someone feels heard, something shifts.
- Vaidi Plovie
Despite these barriers, Eleonora has seen signs of progress. “In the eight years I’ve been studying endometriosis, I’ve noticed a real shift,” she says. “There’s growing awareness among doctors and the general public, and that’s incredibly encouraging.”
Yes, there is more attention than before, and that is hopeful. But awareness still feels fragile. It often depends on moments — a campaign, a story, a specific month — and then it fades again. For those living with endometriosis, it doesn’t fade. It’s there every single day. On a daily basis, we receive messages from people who are searching for answers, recognition, or simply someone who understands.
- Vaidi Plovie
Following her own diagnosis in 2018, Vaidi Plovie founded Endo.Insideout, the Flemish patient organization for people with endometriosis.
The organization provides answers, guidance, organizes events, awareness campaigns, and creates opportunities for people to connect with others who truly understand what they are going through. They continue to advocate for better care through collaboration with healthcare professionals and by contributing to broader discussions around policy and care pathways.
People can easily reach them via social media or their website.
Bethan Burnside